
Prism Glasses vs Vision Therapy: What Is the Difference?
- Vision & Learning Center

- May 19
- 6 min read
Prism glasses and vision therapy are not the same, even though both may be recommended when a patient has binocular vision symptoms.
That matters because families and adult patients are often trying to decide between two very different approaches. One approach may help compensate for the problem. The other may help treat the underlying visual dysfunction. Sometimes one is clearly the better fit. Sometimes both have a role. But they are not interchangeable.
In general, prism glasses are designed to reduce the visual demand on the system by shifting the image and making it easier for the eyes to work together. Vision therapy is designed to improve how the visual system functions by building skills such as eye teaming, tracking, focusing, and binocular control. The AOA’s clinical guideline on accommodative and vergence dysfunction says these disorders often respond to lenses, prisms, or vision therapy, and the National Eye Institute notes that prism glasses can sometimes be used as part of treatment for convergence insufficiency.
What prism glasses are designed to do
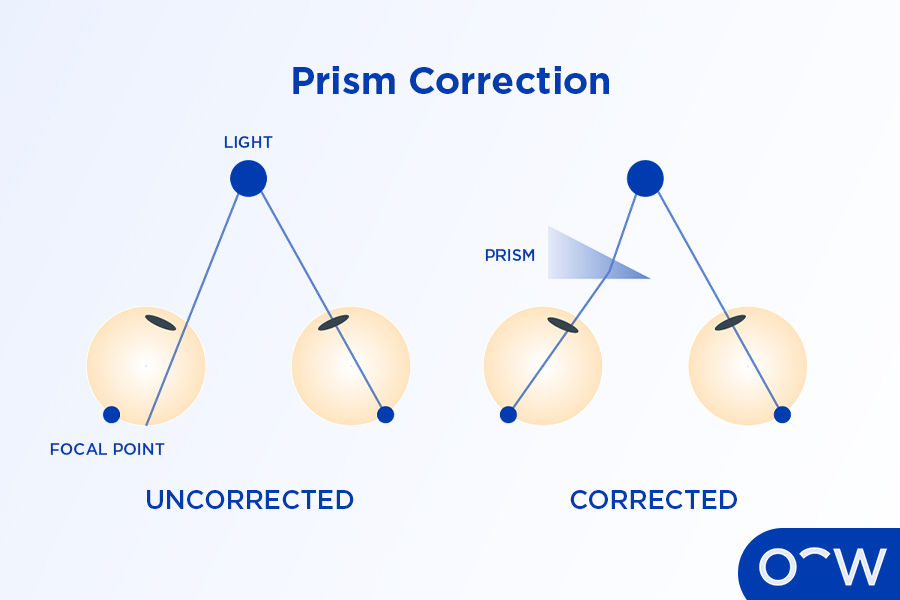
Prism glasses are meant to change how light enters the eyes, so the visual system does not have to work as hard to line things up. In practical terms, a prism is often used to reduce symptoms such as double vision, eyestrain, headaches, or visual discomfort in patients with binocular vision problems. The AOA strabismus guideline says prism may be used for small to moderate deviations, and NEI states that prism glasses are sometimes used in treating convergence insufficiency.
That is why a prism can sometimes provide relatively quick symptom relief. If a patient is symptomatic because the eyes are struggling to maintain alignment or comfortable fusion, prism may reduce that demand. In that sense, a prism is often a supportive or compensatory tool. It can be very helpful, but it is not the same thing as training the system to perform differently on its own. This “compensation versus rehabilitation” distinction is an inference based on how NEI and AOA describe prism as one treatment option among several, rather than as a universal cure for binocular dysfunction.
What vision therapy is designed to do
Vision therapy is designed to improve the function of the visual system itself. The AOA defines optometric vision therapy as a sequence of neurosensory and neuromuscular activities individually prescribed and monitored by a doctor of optometry. Its purpose is to develop or improve visual skills and processing needed for more effective visual performance.
That means vision therapy is not just about helping the patient feel better in the moment. It is aimed at improving how the eyes and brain work together over time. Depending on the diagnosis, that may include work on convergence, accommodation, eye movements, binocular stability, suppression, and visual stamina. NEI describes convergence insufficiency treatment as a type of vision therapy that involves convergence exercises, often with both office- and home-based work.

How these approaches differ
The simplest way to think about it is this:
Prism helps shift the visual demand. Vision therapy helps build visual ability.
That does not mean prism is “bad” or that therapy is always the only right answer. It means they solve different problems.
Prism is often used when symptom relief is needed, when the patient has diplopia or significant discomfort, or when a doctor determines that reducing the demand on the visual system is the right next step. Vision therapy is used when the goal is to improve the underlying binocular or accommodative dysfunction rather than only support it optically. The AOA guideline explicitly includes both prisms and vision therapy among accepted treatment options for accommodative and vergence dysfunction.
When a prism may be considered
Prism may be considered when a patient has:
double vision
decompensated binocular vision symptoms
small to moderate strabismic deviation
convergence insufficiency symptoms
persistent visual discomfort, where reducing demand may help
a situation where immediate symptom relief is especially important
AAO and NEI sources both describe prism as a recognized option in binocular vision care, especially where symptoms relate to alignment or convergence demand.
From a practical standpoint, many clinicians are often more comfortable using prism in adults when the goal is relief of diplopia, reduction of eyestrain, or support for a system that may not be easily changed as quickly. That is a clinical philosophy point, not a universal rule, but it is a useful way to think about how prism is often positioned in real-world care.

When therapy may be considered
Vision therapy may be considered when the goal is not just to relieve symptoms but to improve the way the visual system functions.
That often includes patients with:
convergence insufficiency
accommodative dysfunction
oculomotor problems
binocular instability
visual discomfort with reading or near work
suppression-related binocular problems
some amblyopia- or strabismus-related functional deficits, depending on the case
The strongest evidence base is for office-based vergence/accommodative therapy in symptomatic convergence insufficiency, and AOA guidance describes vision therapy as part of treatment for a broader range of binocular and accommodative disorders.
In children, especially, many binocular vision problems are long-standing and do not simply disappear on their own. In those cases, it often makes more sense to try to strengthen and stabilize the system rather than immediately defaulting to a long-term compensatory approach. In our practice philosophy, that is one reason we are generally more cautious about relying on prism alone in children unless there is a specific reason it is the best fit.
Can a patient ever use both?
Yes.
A patient can absolutely use both prism glasses and vision therapy. In some situations, a prism may help reduce symptoms enough that the patient can function more comfortably while treatment is underway. In other cases, a prism may be used diagnostically, temporarily, or as part of a broader plan. AOA materials on vision therapy and neuro-rehabilitation note that therapeutic lenses may be used for long-term stability in some cases, and AOA’s broader clinical guidance includes both optical and therapy-based treatment approaches.
So this is not always an either-or decision. The real question is: what is the diagnosis, what is the treatment goal, and which approach best matches that goal?
Why evaluation matters before deciding
This is the most important part.
You cannot decide intelligently between prism glasses and vision therapy without knowing what kind of binocular vision problem is actually present.
Two patients may both complain of headaches and reading discomfort, but one may have convergence insufficiency, another may have accommodative dysfunction, another may have a small strabismic deviation, and another may have a more complex sensory-motor binocular problem. Those are not all the same case, so they should not all get the same treatment. NEI also points out that a regular eye exam may not catch convergence insufficiency, even in someone with otherwise “perfect” vision.
That is why the evaluation comes first. The goal is not to pick the option that sounds easiest.
The goal is to pick the option that actually fits the problem.
Frequently asked questions
Are prism glasses and vision therapy the same thing?
No. Prism glasses are an optical treatment that can reduce visual demand or relieve symptoms. Vision therapy is a rehabilitation approach designed to improve visual function.
Do prism glasses fix the problem?
Sometimes a prism is used as a long-term solution, and sometimes it is used more as a compensatory tool. Whether it is the right long-term answer depends on the diagnosis, symptoms, and treatment goals. That distinction is a clinical judgment call made after evaluation, not a one-size-fits-all rule. The guideline-supported point is that prism is a legitimate treatment option for certain binocular disorders.
Is vision therapy better than prism glasses?
Not automatically. They do different jobs. If the goal is immediate symptom reduction, prism may be very helpful. If the goal is to improve underlying binocular function, therapy may be the better fit. Sometimes both are used.
Why are you more cautious with the prism in children?
Because many children with binocular vision problems are dealing with systems that still need to be developed, strengthened, and stabilized. In our practice, we usually prefer to treat the underlying dysfunction when possible rather than relying on compensation alone, unless specific circumstances make prism the better choice.
Are prism glasses more reasonable for adults?
Often, yes. In adults, especially those with persistent diplopia, long-standing decompensation, or situations where symptom relief is a major priority, prism may have a more immediate and practical role. But the right answer still depends on the diagnosis.

Prism glasses and vision therapy are both valuable tools. They are just not the same tool.
Prism is often used to reduce the visual system's workload and help the patient function more comfortably. Vision therapy is used to improve the system's performance. For some patients, especially adults, prism may be the most appropriate answer or part of the answer.
For many children, we are usually more interested in fixing the underlying binocular problem whenever possible rather than settling too quickly for compensation alone.
That is why the first step is always the evaluation. Before deciding between prism, therapy, or both, the most important question is: what problem are we actually treating?



Comments